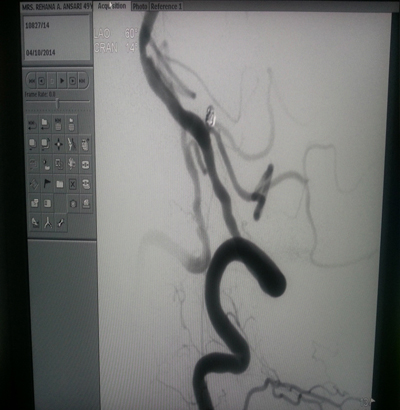
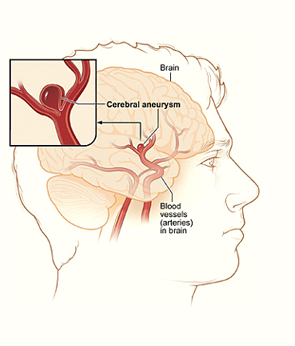
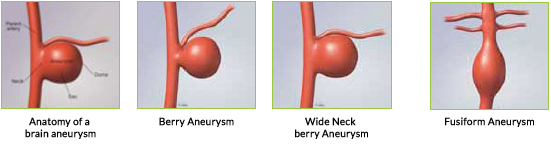
 A brain aneurysm is a weak, bulging spot on the side of a brain artery very much like a thin balloon. Saccular or “berry” aneurysms are the most common type of brain aneurysm. Fusiform aneurysm are less common and are defined by widening of brain artery on both sides. They do not have a defined neck.
A brain aneurysm is a weak, bulging spot on the side of a brain artery very much like a thin balloon. Saccular or “berry” aneurysms are the most common type of brain aneurysm. Fusiform aneurysm are less common and are defined by widening of brain artery on both sides. They do not have a defined neck.
Aneurysms which have bled are called ruptured aneurysms. When the aneurysm ruptures, the blood from the aneurysm usually goes into subarachnoid space , this type of bleed is called a subarachnoid hemorrhage. Rupture of an aneurysm usually causes a sudden severe headache described as the “worst headache of your life”. Other signs of subarachnoid hemorrhage are severe nausea and vomiting, stiff neck and even loss of consciousness.
Unruptured aneurysms may be found by chance on tests performed for other problems such as headaches On occasion, unruptured aneurysms may grow large and press on brain nerves causing problems such as double vision, drooping eyelid, or pain behind the eye. Rarely do unruptured aneurysms cause chronic headaches.

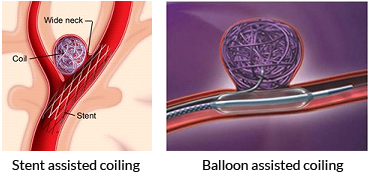

coiling.Newer methods like Balloon Assisted and Stent assisted coiling are used to treat aneurysms with wide necks which would otherwise need open surgeryRecent advances like the Flow Diverter Device, which is a pipeline that redirects blood flow away from the aneurysm are available to treat giant, fusiform and very wide necked aneurysms. 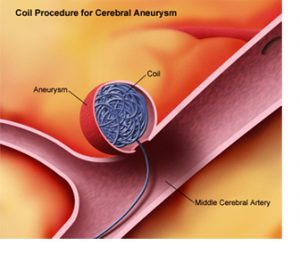
Subarachnoid haemorrhage causes normal cerebral arteries to come in contact with blood. This causes cerebral vasospasm. This means the blood vessels of the brain contract and become narrow. This can be prevented by giving the “HHH” therapy, which included Hypertension, Hemodilution and Hypervolemia. This therapy is initiated as soon as the aneurysm is secured so as to prevent the arteries from going into spasm. This is most common during the 5th to 10th days after first onset of bleeding. If vasospasm does occur, it is treated by giving an oral and or intra-arterial injection of Nimodipine, this is a vasodilator and is injected via a catheter in the brain arteries ( done in the Cath-Lab).
Aneurysm coiling is a relatively safe procedure, and is as effective as surgical clipping in terms of regrowth of the aneurysm.Results of coiling are better than surgical clippingISAT Trial (International subarachnoid Aneurysm trial)
Randomized, prospective, international controlled trial compared neurosurgical clipping with endovascular treatment in aneurysms and concluded that results of coiling were better than surgical clipping.
The early survival advantage was maintained for up to 7 years and was significant.
BRAT Trial (The Barrow Ruptured Aneurysm Trial)
Endovascular coil embolization is superior to microsurgical clipping